Live Longer with Yoga and Meditation
By John M. de Castro, Ph.D.
“A growing body of research supports the immediate benefits of meditation, such as reduced stress and anxiety levels, lower blood pressure, and enhanced happiness. While these initial perks may be reason enough for us to practice, meditation’s positive impact appears to be even more far-reaching, potentially adding years to our lives and improving cognitive function well into old age.” – Rina Deshpande
One of the most exciting findings in molecular biology in recent years was the discovery of the telomere. This is a component of the DNA molecule that is attached to the ends of the strands. Recent genetic research has suggested that the telomere and its regulation is the biological mechanism that produces aging. It has been found that the genes, coded on the DNA molecule, govern cellular processes in our bodies. One of the most fundamental of these processes is cell replication. Cells are constantly turning over. Dying cells or damaged are replaced by new cells. The cells turn over at different rates but most cells in the body are lost and replaced between every few days to every few months. Needless to say, we’re constantly renewing ourselves.
As we age the tail of the DNA molecule called the telomere shortens. When it gets very short cells have a more and more difficult time reproducing and become more likely to produce defective cells. On a cellular basis, this is what produces aging. As we get older the new cells produced are more and more likely to be defective. The shortening of the telomere occurs each time the cell is replaced. So, slowly as we age it gets shorter and shorter. This has been called a “mitotic clock.” This is normal. But, telomere shortening can also be produced by oxidative stress, which can be produced by psychological and physiological stress. This is mediated by stress hormones and the inflammatory response. So, chronic stress can accelerate the aging process. In other words, when we’re chronically stressed we get older faster.
Fortunately, there is a mechanism to protect the telomere. There is an enzyme in the body called telomerase that helps to prevent shortening of the telomere. It also promotes cell survival and enhances stress-resistance. Research suggests that processes that increase telomerase activity tend to slow the aging process by protecting the telomere. One activity that seems to increase telomerase activity and protect telomere length is mindfulness practice. Hence, engaging in mindfulness practices may protect the telomere and thereby slow the aging process.
In today’s Research News article “Impact of Yoga and Meditation on Cellular Aging in Apparently Healthy Individuals: A Prospective, Open-Label Single-Arm Exploratory Study.” See summary below or view the full text of the study at: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5278216/
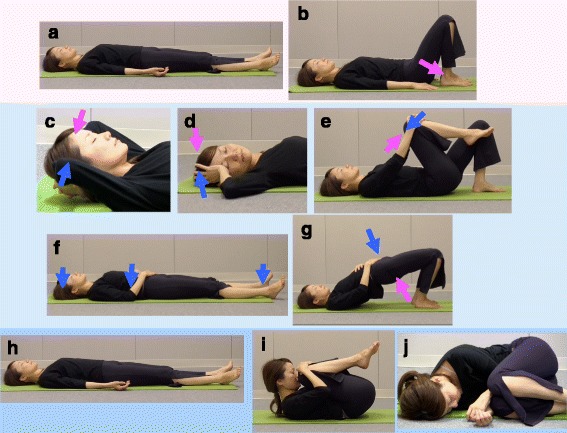
Tolahunase and colleagues examined the effects of a program of yoga and meditation on biomarkers of cellular aging in a healthy population. They recruited healthy adults, aged 35-65 years who led modern sedentary lifestyles and provided them with a 12-week program of Hatha and Raja yogic meditation, breathing exercises, and postures. Sessions were held five days per week for 90 minutes. Participants were measured before and after treatment for a variety of biomarkers of cellular aging.
They found that at the end of the 12-week program there were significant reductions in the levels of the oxidative stress and inflammatory response related biomarkers 8-OH2dG, ROS, cortisol, and IL-6suggesting a reduction in chemical activity that tends to increase cellular aging. They also found that there were significant increases in TAC a marker of antioxidant activity, and markers of cellular aging of telomerase activity, an enzyme that protects the telomeres, β-endorphin, BDNF, and sirtuin-1. Hence, they found clear evidence that the meditation and yoga program greatly reduced the underlying biochemical processes of cellular aging in an otherwise healthy group of adults.
It should be mentioned that there wasn’t a control condition, particularly one that included light exercise. So, it cannot be determined if the results were due to participant expectancies, experimenter bias, attentional effects, the effects of exercise in a sedentary population, or many other potential confounding factors. A randomized controlled clinical trial including a group engaging in light exercise is needed to clarify the causal factors involved. Regardless of the explanation, this study demonstrated that the yoga and meditation program resulted in improvements in biomarkers that suggest that there was a slowing of the processes of cellular aging that underlie the aging of the body. This suggests that engaging in this or similar programs may lead to a longer, healthier life.
So, Live Longer with Yoga and Meditation.
“Yoga and meditation are well-documented to have psychological, emotional and physical benefits for people at all stages of health, including cancer patients. Now breakthrough research reveals yoga and meditation can positively affect DNA.” – Elaine Gavalas
CMCS – Center for Mindfulness and Contemplative Studies
This and other Contemplative Studies posts are also available on Google+ https://plus.google.com/106784388191201299496/posts and on Twitter @MindfulResearch
Study Summary
Tolahunase, M., Sagar, R., & Dada, R. (2017). Impact of Yoga and Meditation on Cellular Aging in Apparently Healthy Individuals: A Prospective, Open-Label Single-Arm Exploratory Study. Oxidative Medicine and Cellular Longevity, 2017, 7928981. http://doi.org/10.1155/2017/7928981
Abstract
This study was designed to explore the impact of Yoga and Meditation based lifestyle intervention (YMLI) on cellular aging in apparently healthy individuals. During this 12-week prospective, open-label, single arm exploratory study, 96 apparently healthy individuals were enrolled to receive YMLI. The primary endpoints were assessment of the change in levels of cardinal biomarkers of cellular aging in blood from baseline to week 12, which included DNA damage marker 8-hydroxy-2′-deoxyguanosine (8-OH2dG), oxidative stress markers reactive oxygen species (ROS), and total antioxidant capacity (TAC), and telomere attrition markers telomere length and telomerase activity. The secondary endpoints were assessment of metabotrophic blood biomarkers associated with cellular aging, which included cortisol, β-endorphin, IL-6, BDNF, and sirtuin-1. After 12 weeks of YMLI, there were significant improvements in both the cardinal biomarkers of cellular aging and the metabotrophic biomarkers influencing cellular aging compared to baseline values. The mean levels of 8-OH2dG, ROS, cortisol, and IL-6 were significantly lower and mean levels of TAC, telomerase activity, β-endorphin, BDNF, and sirtuin-1 were significantly increased (all values p < 0.05) post-YMLI. The mean level of telomere length was increased but the finding was not significant (p = 0.069). YMLI significantly reduced the rate of cellular aging in apparently healthy population.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5278216/